When “No Symptoms” Means No Care: How Asymptomatic STIs Expose Cracks in Women’s Health Care Access
“How would I even know if I had an STI?”
It’s a question many women ask, or perhaps more women should be asking. Sexually transmitted infections (STIs) are often associated with obvious symptoms like abnormal discharge, itching, pain during urination or sex, or visible sores. However, many women with STIs don’t experience these signs. Some of the most common STIs are asymptomatic, meaning they cause few or no noticeable symptoms while still affecting the body. These “silent” infections can persist for months or even years, quietly increasing the risk of serious health consequences, including pelvic inflammatory disease, chronic pelvic pain, infertility, and complications during pregnancy.
Asymptomatic STIs occur for several reasons. The immune system may suppress symptoms without clearing the infection, or symptoms may be mild enough to be mistaken for everyday issues like irritation or fatigue. When the body doesn’t clearly signal that something is wrong, many women delay seeking care, not because they are careless, but because there is no obvious reason to visit a doctor or request testing.
However, the absence of symptoms is only one piece of a much larger problem. Asymptomatic STIs do not become dangerous solely because women fail to seek screening; they become dangerous because preventive sexual health care is often inaccessible, unaffordable, stigmatized, or deprioritized. Even when women are proactive about their health, barriers such as lack of insurance coverage, high out-of-pocket costs, limited clinic availability, time constraints, and fear of judgment can make routine screening difficult or impossible. When infections are silent, the health system must be proactive in identifying them, and too often, it is not.
These barriers do not affect all women equally. Women of color, low-income women, and those living in medically underserved communities experience higher rates of STIs while facing fewer opportunities for routine screening and timely treatment. In this way, asymptomatic STIs reveal not just a biological vulnerability, but a structural failure in how women’s health care is designed and delivered.
Common Asymptomatic STIs: What They Are and Why They’re Often Missed
1. Chlamydia is caused by the bacterium Chlamydia trachomatis and commonly infects the cervix and upper reproductive tract. In women, it often causes little to no noticeable inflammation, which is why more than 70% of infections are asymptomatic. Without testing, chlamydia can persist and increase the risk of pelvic inflammatory disease and infertility.
2. Gonorrhea, caused by Neisseria gonorrhoeae, can infect the cervix, uterus, fallopian tubes, rectum, and throat. Early infection in women frequently produces few or no symptoms, with up to 90% of urogenital infections going unnoticed. Like chlamydia, untreated gonorrhea can ascend into the reproductive tract and cause long-term complications.
3. Genital herpes (HSV) is caused by herpes simplex virus (HSV-1 or HSV-2) and often remains dormant in the body. Many women never experience symptoms or mistake mild symptoms for something else, leaving around 70% unaware they are infected. Even without symptoms, herpes can still be transmitted through asymptomatic viral shedding.
4. Trichomoniasis, caused by the parasite Trichomonas vaginalis, is one of the most common nonviral STIs. Symptoms in women are often mild or absent, with about 85% of infections being asymptomatic. Despite this, untreated trichomoniasis has been linked to pelvic inflammatory disease and increased vulnerability to other STIs.
5. Human papillomavirus (HPV) is extremely common, as 80% of sexually active women will be exposed to HPV at some point in their lives. Most HPV infections cause no symptoms, even when high-risk strains are present. When persistent high-risk HPV goes undetected, it can quietly cause precancerous cell changes that may progress over years to cervical cancer, as well as cancers of the vagina, vulva, anus, and throat, often without warning signs until disease is advanced.
Why Asymptomatic STIs Matter Asymptomatic STIs can have serious consequences for women’s reproductive health. Untreated chlamydia and gonorrhea can lead to pelvic inflammatory disease (PID), which may cause permanent scarring, infertility, ectopic pregnancy, and chronic pelvic pain, even when the original infection was silent. The effects of asymptomatic STIs extend beyond fertility. Persistent HPV infection is the leading cause of cervical cancer, and other infections, including hepatitis B and HIV, are linked to increased cancer risk through chronic inflammation and immune system disruption. Asymptomatic STIs also increase susceptibility to HIV by creating inflammatory environments that facilitate viral transmission.
At the same time, stigma surrounding STIs can take a toll on mental health. Shame, anxiety, and fear of judgment may discourage women from seeking testing or care, and for many, the emotional burden of a diagnosis, or the fear of one, can be just as impactful as the physical effects.
Prevention and Early Detection
Prevention and early detection require more than individual awareness, they require systemic change. Routine STI screening should be treated as a standard component of preventive health care, not an optional or stigmatized service. Normalizing sexual health conversations in primary care settings can help ensure infections are identified before complications arise, particularly for asymptomatic patients.
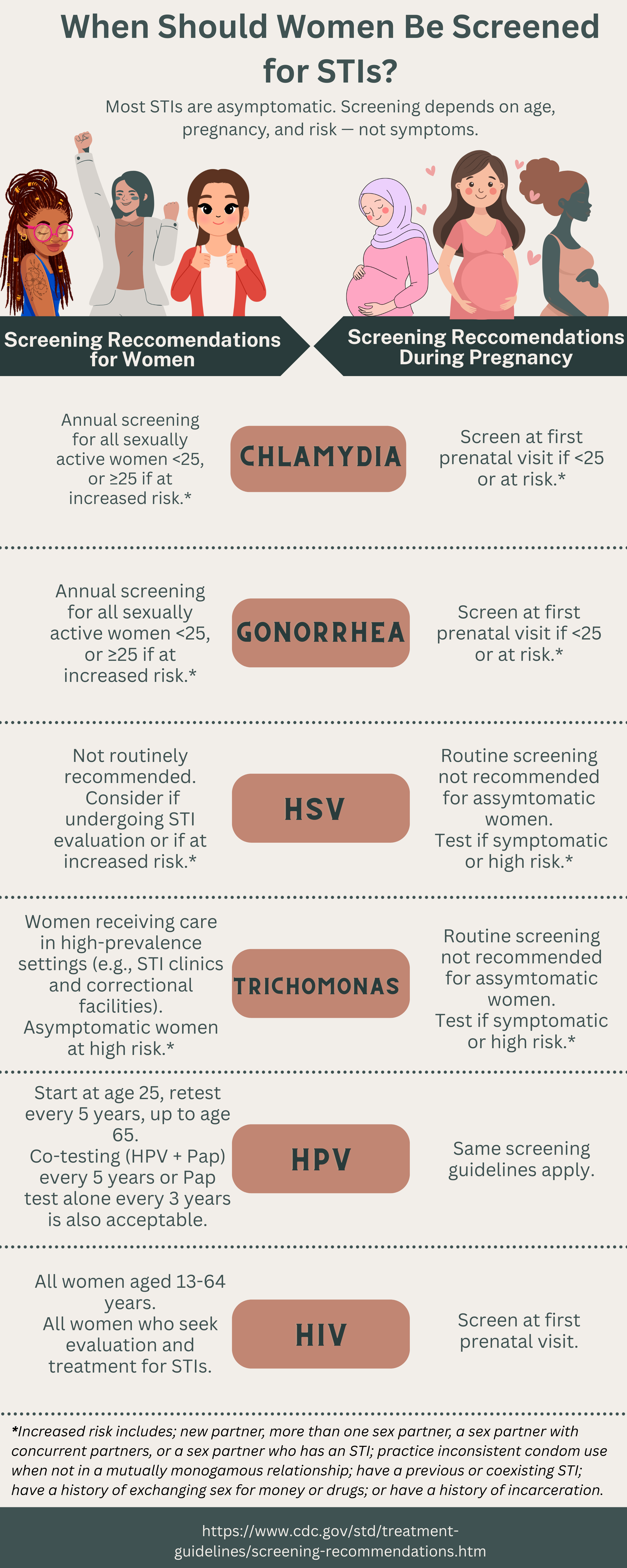
The figure “When Should Women Be Screened for STIs?” summarizes the current screening guidelines from the Centers for Disease Control and Prevention (CDC), including recommendations for women and pregnant women across the most common STIs. As shown in the figure, screening is based on age, pregnancy status, and risk factors, not the presence of symptoms. These guidelines make it clear that screening for many common STIs is intended to be routine and preventive, regardless of accessibility to testing centers and obvious signs of symptoms. This reflects a critical reality; because asymptomatic infections are common, preventive care systems must be designed to proactively identify them. When routine screening is inconsistent or inaccessible, silent infections cause long-term harm for women.
Policies that expand insurance coverage for routine STI testing, eliminate cost-sharing for preventive sexual health services, and support access to care in underserved communities are critical to reducing disparities. HPV vaccination should be offered widely and without stigma, logistical barriers, or unnecessary parental obstacles that delay protection. When preventive care is accessible, normalized, and proactive, asymptomatic infections become far less dangerous.
Conclusion
Asymptomatic STIs are common, particularly among women, and silence does not equal safety. When infections go unnoticed, the consequences can be lifelong, but these outcomes are not inevitable. They reflect gaps in access, inequities in care, and missed opportunities for prevention. Normalizing routine sexual health screening as a standard part of preventive care, expanding access to affordable testing and vaccination, and removing stigma from STI conversations are essential steps toward protecting women’s reproductive health and long-term well-being. Addressing asymptomatic STIs is not just a matter of individual responsibility, it is imperative to public health and health equity.